Be an Advocate for Non-Opioid Postsurgical Pain Control
You’ve always done all you can for your patients. They trust you to listen to them and take their pain seriously. Now show them the difference a multimodal postsurgical pain management approach with EXPAREL can make for their recovery goals.
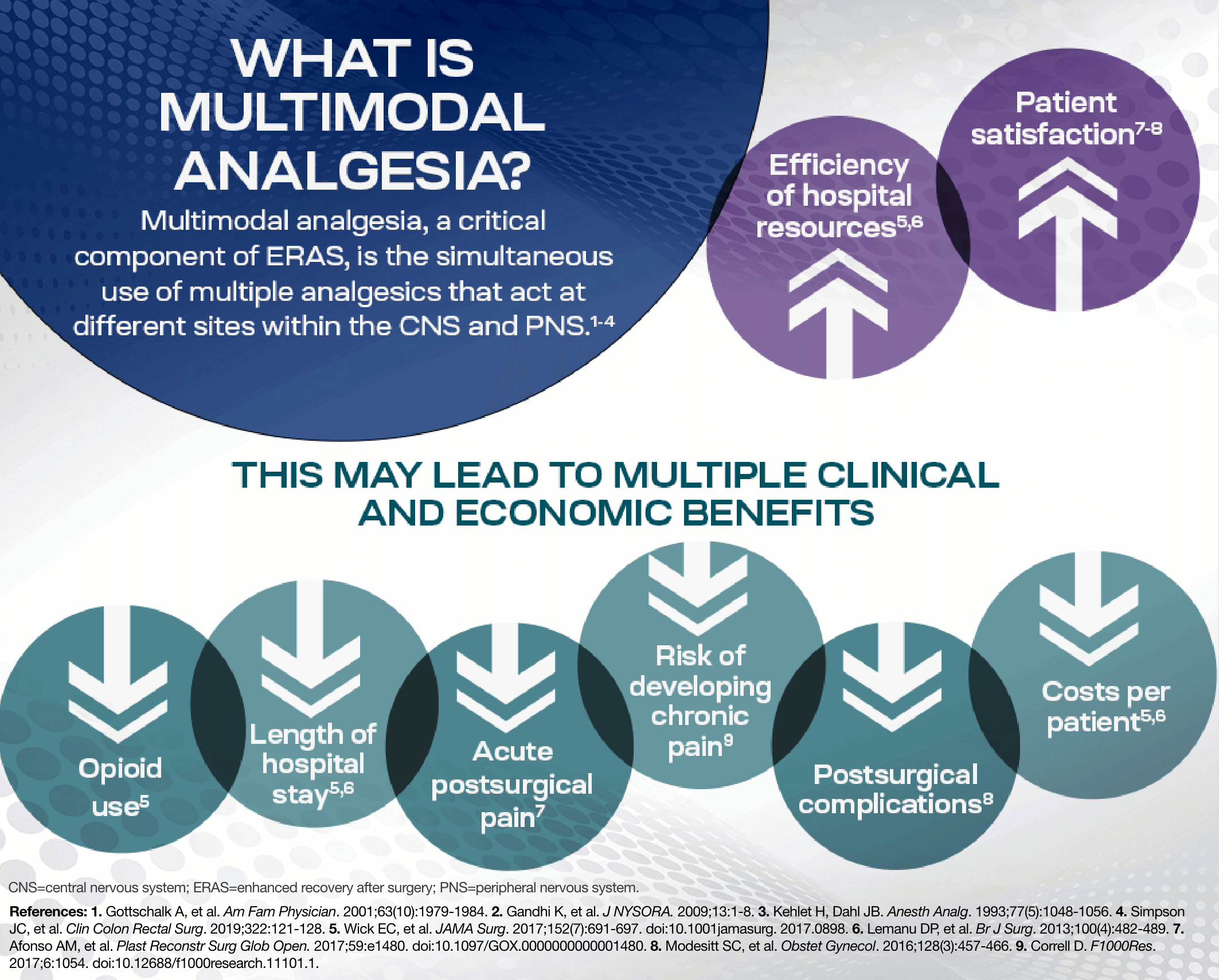
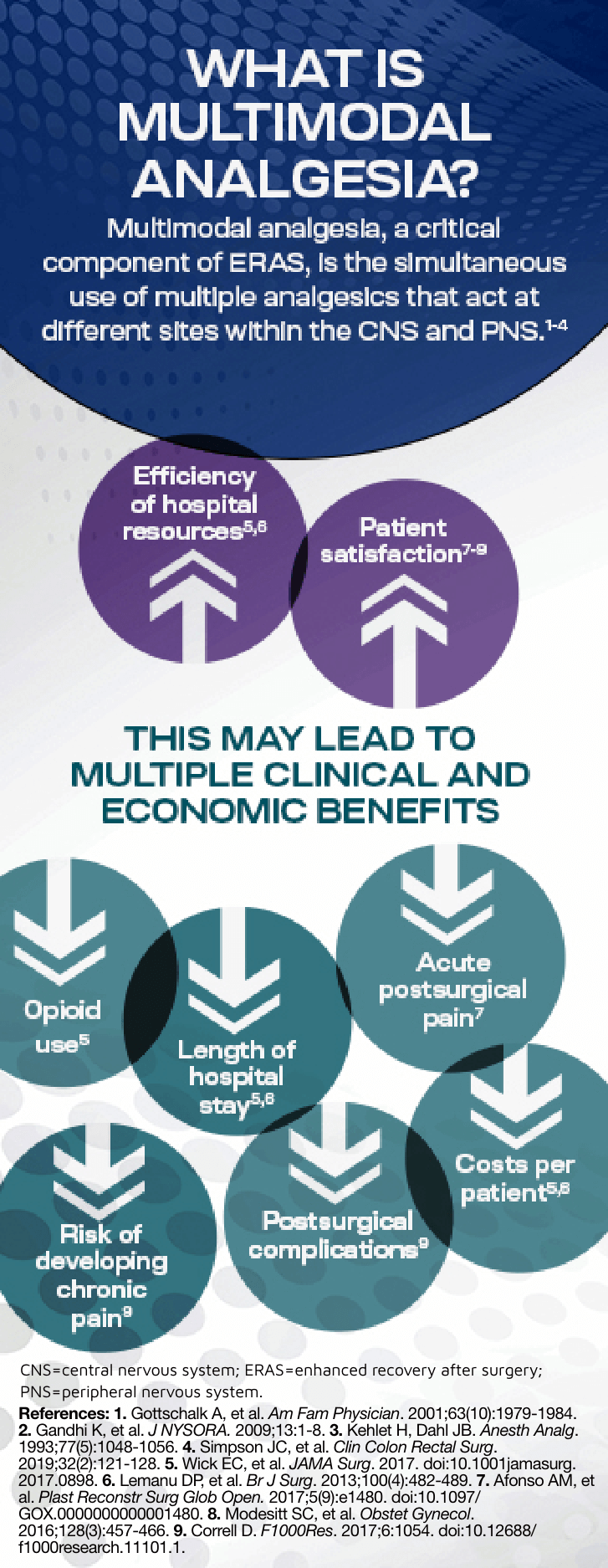
- Enhanced recovery after surgery (ERAS) guidelines recommend a multimodal approach to postsurgical pain management, including less reliance on opioids1
- Multimodal analgesia is the use of multiple pain management modalities for more effective pain control, which can lead to enhanced clinical and economic benefits2
- As the foundation of a multimodal approach, non-opioid EXPAREL can help reduce—or even eliminate—the use of postsurgical opioids, while providing the pain control patients need3*
To minimize postsurgical pain with EXPAREL, download the Nursing Guide.
*The clinical benefit of the decrease in opioid consumption was not demonstrated in the pivotal trials.
Get a Nurse's Perspective
TALK NURSE TO NURSENURSES ARE THE
MOST TRUSTED
PROFESSIONALS
For the past 20 years, nursing has been the top-ranked profession for high honesty and ethics.4†
†Annual Gallup rating of the honesty and ethics of various professions.
Why do patients trust nurses so strongly?
THEY LISTEN
95%
of patients say listening to them is critical5‡
‡Beryl Institute survey of what health care consumers consider to be
extremely important to their experience.
Your role in implementing the ERAS plan is critical
Inadequate pain management after surgery can lead to unintended consequences for your patients—from chronic pain to extended hospital stays. In addition, postsurgical pain significantly contributes to patient dissatisfaction with the anesthesia and surgical experience.6
ERAS protocols help improve key postsurgical outcomes by significantly reducing7§
Pain scores within the first 24 hours of surgery
Opioid consumption for the first 48 hours after surgery
Hospital LOS from admission to discharge
§Data shown are from colorectal surgery.
Teamwork is key to ERAS pathway success
Nurses
Surgeons
Anesthesiologists
Administrators
As a nurse, your role in the multidisciplinary ERAS team includes
- Providing essential patient education for each step of the surgical care experience: preoperative, intraoperative, and postoperative8
- Assessing the patient’s pain level and tolerance9
- Facilitating communication between the physician and the patient9
- Informing caregivers about the patient’s status8,9
LOS=length of stay.
Contact a Clinical Educator for ERAS support
CONNECT WITH USAvoid the complications of opioids
Opioid-related adverse events (ORAEs) can add to your workload. With the growing number of patients you’re caring for, you shouldn’t have to contend with patients who are:
- Sick from ORAEs like nausea and vomiting6,10
- Slow to ambulate due to light-headedness and oversedation11
- Having difficulty breathing due to respiratory depression6
- Experiencing discharge delays due to ORAEs12
- Complaining of discomfort with opioids, such as pruritus6
Fortunately, there are non-opioid postsurgical pain management options to help you. If additional pain relief is needed after surgery, patients should receive an around-the-clock regimen of NSAIDs, COX inhibitors, and/or acetaminophen (unless contraindicated).13,14
You can help minimize opioid use by advocating for a multimodal pain management approach that includes EXPAREL with both the physician and the patient:
- Inform patients about multimodal approaches and non-opioid pain management options
- Empower patients to speak up and ask the physician for non-opioid options
- Share the ORAEs you see with the prescribing physician
Download a handout to help your patients manage postsurgical pain with minimal opioid use.
Nurses are stewards for opioid administration
If you are administering pain management medications following surgery, consider the patient types who may react differently to opioids.
For example:
- Opioid-naive patients may not realize the impact of opioids extends beyond pain control10
- Educate them on the side effects of and risks of opioids: abuse, addiction, and diversion15
- Provide safe disposal instructions15
- Patients with a history of opioid or substance use disorder14
- Confirm if patients need non-opioid pain medication to avoid the risk of relapse that may compromise their sobriety
National Nursing Societies Agree on Limiting Opioid Use
AORN
“When leveraged effectively, multimodal analgesia can be an integral part of improving the surgical patient experience, improving pain control and solving the opioid crisis.”16
ASPAN
“…opioids now require careful governance and judicious utilization.”17
ASPMN
“…prescribing and administering doses of opioid analgesics based solely on a patient’s pain intensity should be prohibited”18
AWHONN
“Nurses should be competent in screening approaches to identify the use of legal and illegal substances and SUD in pregnant women and women who may become pregnant.”19
NAON
“The use of multimodal analgesia and an alternative method of pain control can be highly effective and can decrease burdens of opioid use on patients and their families.”20
AORN=Association of periOperative Registered Nurses; ASPAN=American Society of PeriAnesthesia Nurses; ASPMN=American Society for Pain Management Nursing; AWHONN=Association of Women’s Health, Obstetric, and Neonatal Nurses; COX=cyclooxygenase; LOS=length of stay; NAON=National Association of Orthopaedic Nurses; NSAID=non-steroidal anti-inflammatory drug; SUD=substance use disorder.
The first few days after surgery can be the most painful for patients
One of the most critical opportunities with ERAS protocols is postsurgical pain management2,10,21
- Optimizing pain management after surgery can positively impact factors such as ambulation, reducing LOS, and reducing opioids
- Pain relief remains an unmet need:
75% to 88% of patients report moderate to extreme postsurgical pain6
Nearly 80% of patients preferred a non-opioid postsurgical pain management option22
EXPAREL can provide long-lasting, non-opioid pain relief for your patients:
- When used as part of a multimodal protocol, EXPAREL aligns with ERAS guidelines by reducing the need for opioids in both adults and children 6 years of age or older, as demonstrated in clinical trials23§
- The benefits of EXPAREL start during the surgical procedure and continue for days after your patients arrive home
- ERAS and multimodal protocols with EXPAREL can help lessen your burden24
- Decreases the time you need to attend to each patient after surgery
- Reduces follow-up calls after discharge
- Improves patient satisfaction scores
24 hours after surgery for knee OA25:
85%
of patients were satisfied with EXPAREL pain control
vs
69%
of patients who did not receive EXPAREL
A phase 4, multicenter, double-blind, active-controlled, parallel-group trial in which patients were randomized 1:1 to receive local infiltration analgesia with EXPAREL (n=70) or bupivacaine HCl alone (n=69; P=0.036).
Optimize Patient Experience With EXPAREL
1

During surgery2
EXPAREL is administered during surgery and works directly at the site to provide targeted analgesia.
2

After surgery24,26
Unlike PCA, EXPAREL controls pain while minimizing the need for opioids without pumps or catheters. Less opioid use reduces the risk of opioid-related side effects that can hinder the achievement of key recovery milestones (eg, time to first bowel movement or flatus, eating solid foods, ambulation, and discharge).
3
At home27
With up to 72 hours of pain control, EXPAREL helps patients recover without the side effects of opioids.
§The clinical benefit of the decrease in opioid consumption was not demonstrated in the pivotal trials.
ERAS=enhanced recovery after surgery; LOS=length of stay; PCA=patient-controlled analgesia.
Most Valuable EXPAREL Resources for Nurses
Access the EXPAREL resources that most nurses depend on.
 View
View